

World Without Cancer
a book by Edward Griffin
[Chapter 1] THE WATERGATE SYNDROME
[Chapter 8] THE LAETRILE "QUACKS"
[Chapter 10] The Hoax Of The "Proven" Cancer Cures by G. Edward Griffin
=====================
Chapter 1
THE WATERGATE SYNDROME
from World Without Cancer by Edward Griffin
Examples of dishonesty and corruption in the field of drug research; a close look at the first major study which declared Laetrile) vitamin B-17) “of no value;” proof that the study was fraudulent; the FDA’s ruling against the use of Laetrile because it had not been tested; and the refusal then to allow anyone (except its opponents) to test it.
This year 550,000 Americans will die from cancer. One out of three of us will develop cancer in our lifetime. That is eighty-eight million people in the United States alone.
The purpose of this study is to show that this great human tragedy can be stopped now entirely on the basis of existing scientific knowledge.
We will explore the theory that cancer, like scurvy or pellagra, is a deficiency disease aggravated by the lack of an essential food compounds in modern man’s diet, and that its ultimate control is to be found simply in restoring this substance to our daily intake.
What you are about to read does not carry the approval of organized medicine. The Food and Drug Administration, the American Cancer Society, and the American Medical Association have labelled it fraud and quackery. In fact, the FDA and other agencies of government have used every means at their disposal to prevent this story from being told. They have arrested citizens for holding public meetings to tell others of their convictions on this subject. They have confiscated films and books. They even have prosecuted doctors who apply these theories in an effort to save the lives of their own patients.
The attitude of Big Brother, expressed bluntly in 1971 by Grant Leake, Chief of the fraud section of California’s food and drug bureau, is this: “We’re going to protect them even if some of them don’t want protection.” [1]
Early in 1974, the California medical board brought formal charges against Stewart M. Jones, M.D., for using laetrile in the treatment of cancer patients. It was learned later, however, that Dr. Julius Levine, one of the members of that board, himself had been using Laetrile in the treatment of his own cancer. When Dr. Jones’ case came up for review, the political pressures were so great that Dr. Levine felt compelled to resign from his post rather than come out openly in support of Dr. Jones and his patients. [2]
This is happening in a land which boasts of freedom and whose symbol is the Statue of Liberty. For the first time in our history, people are being forced to fell from our shores as medical emigrants seeking freedom-of choice and sovereignty over their own bodies. Laetrile has been available in Australia, Brazil, Belgium, Costa Rica, England, Germany, Greece, India, Israel, Italy, Japan, Lebanon, Mexico, Peru, the Philippines, Spain, Switzerland, Russia, Venezuela, and Vietnam-but it is not allowed in the “land of the free”
In spite of this, however, many doctors have defied the bureaucracy and have proved in ther own clinics that vitamin-deficiency concepts of cancer is valid.
With billions of dollars spent each year in research, with additional billions taken in from the cancer-related sale of drugs, and with vote-hungry politicians promising ever-increasing government programs, we find that, today, there are more people making a living from cancer than dying from it. If the riddle were to be solved be a simple vitamin, this gigantic commercial and political industry could be wiped outovernight. The result is that the science of cancer therapy is not nearly as complicated as the politics of cancer therapy.
If there was any good that came from the Watergate scandals of the Seventies, it as the public awakening to the reality that government officials sometimes do not tell the truth. And when caught in such “mendacities,” they invariably claim that they lied only to protect national security, public health, or some other equally noble objective.
This Watergate syndrome is not new. Several years ago, an FDA agent who had testified in court against a Kansas City businessman admitted under cross-examination that he had lied under oath twenty-eight times. When asked if he regretted what he had done, he replied: “No. I don’t have any regrets. I wouldn’t hesitate to tell a lie if it would help the American consumer.” [3]
The FDA is not squeamish over its tactics to “help the American consumer.” When a businessman falls into disfavor with the bureaucracy, there are no holds barred, and the law is used, not as a reason for attack, but as a weapon of attack. In other words, the FDA does not take action because the law says it should. It does so because it wants to, and then searches through the law for an excuse. In the celebrated case of U.S. vs Dextra Fortified Sugar, for example, the FDA had ruled that it was “misbranding” to fortify sugar with vitamis and minerals and still call it sugar. But the court ruled otherwise, pointing out:
The basic flaw in the government’s case is that it is seeking, under the guise of misbranding charges, to prohibit the sale of a food in the market place simply because it is not in sympathy with its use.
Usually there is much more going on in these cases than over-zealousness on the part of a few bureaucrats. Pretending to protect the public is the favorite cover for hidden agendas. Legislation claiming to protect the consumer usually is written by representatives of the very industries from which the consumer supposedly is to be protected. Politicians who are grateful for the financial support of those industries are eager to put their names on the legislation and push for its enactment. Once it becomes law, it serves merely to protect the sponsoring industries against competition. The consumer is the victim, not the beneficiary.
This is just as true in the field of medicine as in any other. In medicine, however, there is the added necessity to pretend that everything is being done scientifically. Therefore, in addition to recruiting the aid of politicians, scientists also must be enlisted- a feat that is easily accomplished by the judicious allocation of funding for research.
This reality was revealed by former FDA Commissioner, James L. Goddard in a 1966 speech before the Pharmaceutical Manufacturers Association. Expressing concern over dishonesty in the testing for new drugs, he said:
I have been shocked at the materials that come in. In addition to the problem of quality, there is the problem of dishonesty in the investigational new drug usage. I will admit there are grey areas in the IND [Investigation of New Drug] situation, but the conscious withholding of unfavorable animal clinical data is not a grey matter. The deliberate choice of clinical investigators know to be more concerned about industry friendships than in developing good data is not a grey matter.[4]
Goddard’s successor at the FDA was Dr. Herbert Ley. In 1969, he testified before a Senate committee and described several cases of blatant dishonesty in drug testing. One case involved an assistant professor of medicine who had tested 24 drugs for 9 different companies. Dr. Ley said:
Patients who died while on clinical trials were not reported to the sponsor…Dead people were listed as subjects of testing. People reported as subjects of testing were not in the hospital at the time of tests. Patient consent forms bore dates indicating they were signed after the subjects died. [5]
Another case involved a commercial drug-testing firm that had worked on 82 drugs from 28 companies. Dr Ley continued:
Patients who died, left the hospital, or dropped out of the study were replaced by other patients in the tests without notification in the records. Forty-one patients reported as participating in studies keeping, supervision and observation of patients in general were grossly inadequate. [6]
Between 1977 and 1980, it was discovered that 62 doctors had submitted clinical data to the FDA which was manipulated or completely falsified.[7] In one study conducted by the FDA itself, it was discovered that one in every five doctors investigated- doctors researching the effects of new drugs-had invented the data they reported and pocketed the fees.[8]
These are not unusual or isolated cases. John Braithwaite, a criminologist at the Australian Institute of Criminology (and also former Commissioner of Trade Practices in Austrailia), states: “The problem is that most fraud in clinical trials is unlikely to even be detected. Most cases which do come to public attention only do so because of the extraordinary carelessness by the criminal physician.”[9]
According to Dr. Judith Jones, former Director of the Division of Drug Experience at the FDA, if a research facility obtains results that do not demonstrate the safety or effectiveness of a drug, it is not uncommon for the drug company to bury the report and continue testing elsewhere until they find a facility that gives them the results they want. Unfavorable reports are rarely published, and clinicians are pressured into keeping quiet about them.[10]
The incentive for clinical investigators to fabricate data is enormous. American drug companies pay as much as $1,000 per patient, which enables some doctors to collect over $1 million per year from drug research-all the easier if the treatments are imaginary. Even if the tests are not fabricated, there is still the effect of subconscious bias. These doctors know that, if they don’t produce the results the drug companies are seeking, the likelihood of their receiving future work is greatly diminished.
The commercially operated testing facilities should become corrupted by money is not hard to imagine. But it is often assumed that university laboratories are different, that they are immune to the profits that flow from criminal science. The truth, however, is that money speaks just as loudly on campus as it does elsewhere. Referring to a survey conducted by the FDA, Dr. Braithwaite explains:
As one would predict from the foregoing discussion of how contract labs can be used by sponsors to abrogate responsibility for quality research , contract labs were found to have a worse record of GLP [Good Laboratory Practices] violations that sponsor labs. The worst record of all, however, was with university laboratories. One must be extremely cautious about this finding since there were only five university laboratories in the study. Nevertheless, it must undermine any automatic assumption that university researchers, with their supposed detachment from the profit motive, are unlikely to cut corners on research standards.[9]
Let’s bring this into focus on the issue of cancer. Science can be used, not only to push drugs into the market that do not work, but also to hold back remedies that do-because these remedies represent potential competition to pharmaceutical industry which controls the drug-approving process. The controversy that once surrounded Dr. Andrew Ivy’s anti-cancer drug known as Krebiozen is an example of this phenomenon.
Prior to crossing swords with the FDA in the early 1960’s, Dr. Ivy had been widely acknowledged as one of the nation’s foremost medical specialists. As head of the University of Illinois the graduate degrees of Doctor of Philosophy (Ph.D.) and Master of Science (M.S.). He was an American Representative at the Nuremberg trials after World War II in Germany. The American representative at the Nuremberg trials after World War II in Germany. The American Medical Association had awarded him bronze, silver, and gold medels in recognition of his outstanding work in the field of medicine. He had written over a thousand articles published in scientific and medial journals. In fact, the FDA itself often had called upon him as an expert to offer medical testimony in court. But when he began to use an unorthodox approach to cancer therapy, overnight he was branded as a “quack.”
During the course of Dr. Ivy’s trial, a letter was read into the court record written by a doctor from Indianapolis. The doctor stated in his letter that he was treating a patient who had multiple tumors, and that a biopsy of the tissue had shown these tumors to be cancerous. The doctor said that he had obtained Krebiozen from Dr.Ivy’s laboratories and had administered it, but that it had done absolutely no good. When called to the witness stand, however, the doctor’s answers were vague and evasive. Under the pressure of cross-examination, he finally broke down and admitted that he never had treated such a patient, never had ordered the biopsy in question, and never had used Krebiozen even once. The whole story had been a lie. Why did he give false testimony? His reply was that one of the FDA agents had written the letter and asked him to sign it. He did so because he wanted to help the agency put an end to quackery. [12]
In September of 1963, the FDA released a report to the effect that Krebiozen was, for all practical purposes, the same as creatine, a common substance that was found in every hamburger. To prove this point, they produced a photographic overlay supposedly showing the spectograms of Krebiozen and creatine superimposed over each other. These were published in Life magazine and other segments of the mass communications media as “unimpeachable proof” that Krebiozen was useless.
When Senator Paul Douglas saw the spectrograms, he was suspicious. So he asked Dr. Scott Anderson, one of the nation’s foremost authorities on spectograms, to make his own study. Using standard techniques of analysis, Dr. Anderson identified twenty-nine differences between the two substances. There were sixteen chemical and color differences. The version released to the press by the FDA had been carefully moved off center until there was a maximum appearance of similarity, but when restored to the true axis, the two were as different as night and day.[13]
The tactics used against Laetrile are even more dishonest than those against Krebiozen. Perhaps the most damaging of them has been a pseudo-scientific report released in 1953 by the Cancer Commission of the California Medical Association. Published in the April issue of California Medicine, the report presented an impressive collection of charts and technical data indicating that exhaustive research had been carried out into every aspect of Laetrile. Its molecular Composition had been analyzed, its chemical action studied, its effect on tumor-bearing rats observed, and its effectiveness on human cancer patients determined. The stern conclusion of all the supposedly objective research was stated: “No satisfactory evidence has been produced to indicate any significant cytotoxic effect of Laetrile on the cancer cell.”
The conclusions of the California Report are sufficient for most physicians and researchers. Not one in ten thousand has ever even seen Laetrile, much less used it. Yet, they all know that Laetrile does now work because the California branch of the AMA Cancer Commission said so, and they have had no reason so question the reliability of those who did the work.
Reporter Tom Valentine interviewed many leading cancer specialists to determine what they thought about Laetrile. Here he describes a typical reaction:
Dr. Edwin Mirand of Roswell Memorial Hospital in Buffalo, N.Y. said: “We’ve looked into it and found it has no value.” When asked if the renowned little hospital, which deals only with cancer, actually tested Laetrile, Dr. Mirand said, “No, we didn’t feel it was necessary after others of good reputation had tested it and found had no effectiveness in the treatment of cancer.” He referred, as all authorities do, to the California Report.[15]
Others have run up against the same stone wall. Professional researcher, David Martin, reported this experience:
The cancer expert in question, as I had anticipated, told me that Laetrile was “sugar pills.” Had he told me that he had used Laetrile experimentally on X number of patients and found it completely ineffective, I might have been impressed. But when I asked him whether he had ever used it himself, he said that he had not. When I asked him whether he had ever travelled abroad to study the experience with Laetrile therapy in Germany, Italy , Mexico, the Philippines, or other countries, her replied that he had not. And when I asked him if he had ever made a first-hand study of the pros and cons of the subject, again he conceded that he had not. He was simply repeating what he had heard from others who, in turn , were probably repeating what they had heard from others, going all the way back to the antiquated 1953 report of the California Cancer Commission. [16]
It is important, therefore, to know something of the nature of the California Report and of the scientific integrity of those who drafted it.
Although the report as published in California Medicine was unsigned, it was written by Dr. Ian MacDonaldm, Chairman of the Commission, and Dr. Henty Garland, Secretary. Dr. MacDonald was a prominent cancer surgeon, and Dr. Garland was an internationally famous radiologist. Both were listed in Who’s Who.
There were even seven other prominent physicians on the commission-including four more surgeons, another radiologist, and a pathologist-but they played no major part in the preparation of the report. Not one of these men-not even MacDonald or Garaland-had ever used Laetrile in the first-hand experiments of their own. All they had done was to make evaluations and summaries of the written records of others.
There were even seven other prominent physicians on the commission-including four more surgeons, another radiologist, and a pathologist-but they played no major part in the preparation of the report. Not one of these men-not even MacDonald or Garaland-had ever used Laetrile in the first-hand experiments of their own. All they had done was to make evaluations and summaries of the written records of others.
Before examining those evaluations and summaries, let us first recall that MacDonald and Garland were the two physicians who had made national headlines claiming that there was no connection between cigarette smoking and lung cancer. In an address before the Public Health Section of the Commonwealth Club of San Francisco on July 9, 1964, Dr. Garland had said:
A current widely held hypothesis is that cigarette smoking is causally related to a vast number of different diseases, ranging from cancer to coronary arteriosclerosis. After studying the question for several years, notably in its reported relationship to primary bronchial cancer, it is my considered opinion that the hypothesis is not proven….
Cigarettes in moderation are regarded by many as one of the better tranquilizers…. It is likely that obesity is a greater hazard to American health than cigarettes.
Dr. MacDonald was even more emphatic. In an article in U.S. News & World Report, he was shown with a cigarette in his hand, and is quoted as saying that smoking is “a harmless pastime up to twenty-four cigarettes per day.” And then he added: “One could modify an old slogan: A pack a day keeps lung cancer away.”[17]
It is a curious fact that it was precisely at this time that cigarette manufacturers were beginning to experience a slump in sales because of public concern over lung cancer. In fact, tobacco industry had already pledged the first ten-million dollars out of a total of eighteen million to the AMA for “research” into the question of smoking and health.
The effect of this veritable flood of money from a source with, shall we say, “a vested interest” in the outcome of the research, was incredible and did not speak well for the AMA. The result was the conversion of a relatively simple, straight-forward project into a monstrous boondoggle of confusion and waste.
In the report of the AMA’s Committee for Research on Tobacco and Health, it says:
To date, approximately $14 million has been awarded [from the tobacco industry] to 203 individual research projects at 90 universities and institutions. As a direct result of these grants, 450 reports have been published in scientific journals and periodicals.[18]
The report then listed the research projects and described their purposes. Here are just a few:
Nicotine Receptors in Identified Cells of the Snail Brain.
The Effects of Nicotine on Behavior of Mice.
Angina Pectoris and Bronchitis in Relation to Smoking – A Study in American and Swedish Twin Roosters.
Post – Maturity Syndrome in the Pregnant Rat After Nicotine Absorption During Pregnancy.
Interactions of Nicotine, Caffeine and Alcohol in Squirrel Monkeys.
The Effect of Smoking in Placental Oxygen Transfer in Gravid Ewes.
Urinary Excretion, Tissue Distribution and Destruction of Nicotine in Monkey and Dog.
Body Build and Mortality in 105,000 World War II Army Verterans.
Upon going through the back reports of the AMA’s Committee for Research on Tobacco and Health, one is able to count but five research projects that are primarily concerned with cancer. One of those dealt with laboratory-testing procedures only, and another was an experiment to see if tobacco smoke could be used to cure cancer of the skin! So only three of these projects really dealt with the area of major public concern. Three out of two hundred and three is only about one-and-a-half percent – which tells us something about the AMA’s scientific integrity on the subject of smoking and cancer.
With the expenditure of a mere eighteen-million dollars – which is small, indeed, compared to the tobacco industry’s advertising budges over the same period – it was possible to direct the AMA’s medical research away from the important question of cancer and into a hundred giddy questions that served only to confuse and delay the ultimate truth.
Dazzled by the meteor shower of thousand-dollar bills, the AMA, in its December 1959 issue of the American Medical Association Journal, published an editorial stating flatly that there was insufficient evidence “to warrant the assumption” that cigarette smoking was the principal factor in the increase of lung cancer. Furthermore, through its gargantuan research program, the AMA was making it increasingly difficult to obtain that evidence.
Was there any connection between the eighteen-million dollars given to the AMA from the tobacco industry and the public pronouncements of MacDonald and Garland, two of its most prominent members in California? Perhaps not, although it has been rumored that these gentlemen of science actually did receive $50,000 for their “testimonials.”[19]
Whether or not this is true is not important now. What is important is the fact that their medical opinion, if it had been widely followed, clearly would have resulted in the suffering and death of untold additional millions. Also important is the fact that these are the same “experts” whose medical opinion has been widely quoted and followed in the question of Laetrile.
An interesting footnote to this subject is the fact that Dr. MacDonald was burned to death in bed a few years later in a fire started by his cigarette. Dr. Garland, who had boasted of chain-smoking since early childhood and who claimed to be living proof that cigarettes are harmless, a few years later died of lung cancer.
In 1963, ten years after publication of the original California Report, the California State Department of Health officially decreed that he findings of the antiquated study were “true” and adopted them as its own. When it did so, however, it performed an unexpected favor for the public because it published for the first time all the original experiments and studies upon which the report had been based and, in doing so, it made available the documentary evidence proving that MacDonald and Garland had falsified their summary of those experiments.
In the 1953 report, the authors published the conclusions of John W. Mehl, M.D., to the effect that cyanide could not be released from Laetrile. As will be explained in a later chapter, the release of cyanide at the cancer cell is part of the reason that Laetrile works. Therefore, imlpying that cyanide cannot be produced was a severe blow to the credibility of Laetrile theory. Dr. Mehl was quoted as saying: “These results are inconclusive, and will be extended, but they do not support the claims made for “Laetrile.”
With the publication of the original experiments ten years later, however, quite a different story emerged. Buried in a maze of statistics, tables, and charts can be found an item labeled “Laetrile Report Appendix 4.” It is a laboratory report signed by G. Schroetenboer and W. Wolman. It states:
After refluxing for three hours, the odor of hydrogen cyanide could be detected… The hydrogen cyanide was distilled into sodium hydroxide and determined by the Prussian Blue technique.[20]
This report was dated January 14, 1953 – two months before Dr. Mehl claimed that cyanide could not be released from Laetrile. It is significant, therefore, that MacDonald and Garland completely ignored the positive report while giving prominence to the negative one.
Since that time, the release of cyanide from Laetrile has been confirmed by the AMA’s chemical lab, by the cytochemistry section of the National Cancer Institute, and even by the California Department of Public Health that then officially pronounced the original report to be “true” and adopted it as its own.
Another claim made by Drs. MacDonald and Garland was that microscopic examinations of tumors from patients who had been treated with Laetrile showed absolutely no indication of favorable chemical effect. Ten years later, however, this assertion was shown to be a bald-faced lie. Appendix Three contains the findings of two pathologists who stated in plain English that they did observe anti-tumor effects which, indeed, could have been caused by the Laetrile. In a statement dated December 15, 1952, for example, John W. Budd, M.D., reported: “Case 1M…. Hemorrhagic necrosis of tumor is extensive…. An interpretation of chemotherapeutic effect might be entertained.”
Also an autopsy report by J.L. Zundell, dated September 10, 1952, discusses two clear cases of observed anti-tumor effect. It states:
M-1…. This might represent a chemical effect since the cells affected show coagulation necrosis and pyknosis….
M-3…. There appears to be more degeneration in the tumor cells in the lymph node. I would consider this as a possible result of chemical agent….
Two cases…. Showed moderated changes … which might be considered as chemotherapeutic toxic cellular changes.[21]
Nothing could be more plain than that. Nevertheless, MacDonald and Garland stated flatly in the California Report: “No evidence of cytotoxic changes was observed by any of the consultants.” [22] That statement, of course, was a lie of gigantic proportions.
Even if the findings of these researchers had not been falsely summarized by MacDonald and Garland, the 1953 California Report still would have been totally useless as a scientific verdict against Laetrile because the strength of the doses used on cancer patients was too weak to prove anything. In fact, it was about one-fiftieth (1/50) of what generally is used to obtain optimum results.
In the earlier days of Laetrile research, clinicians cautiously administered only fifty to one-hundred milligrams at a time. Gaining confidence with experience, these levels gradually were raised until, by 1974, Laetrile was being used intravenously at levels of six to nine thousand milligrams daily. Generally, it takes an accumulation of fifty to seventy thousand milligrams over a period of about a week or ten days before the patient can report tangible indications of improvement. But in the experiments used for the California Report, the typical dose given was only about fifty milligrams per infection. The maximum single dose was less than two hundred milligrams, and the maximum accumulative dose was only two thousand milligrams spread over twelve injections. Five patients received only two infections, and five received only one.
It is not surprising, therefore, that the California experiments failed to produce conclusive evidence Laetrile was effective against cancer. As Dr. Krebs observed at the time, “There is nothing quite so easy to accomplish as failure.”
In spite of all the incredible distortions of fat and the perversions of scientific truth, Drs. MacDonald and Garland were forced to admit on page three of their California Report:
All of the physicians whose patients were reviewed spoke of increase in the sense of well-being and appetite, gain in weight, and decrease in pain…
Then, attempting to belittle these important results, they added:
…as though these observations constituted evidence of definite therapeutic effect.
That statement, alone, should have disqualified the California Report, for these observations are, indeed, among the very things which indicate to a physician whether or not his drug therapy is effective.[23] Most doctors would be ecstatically happy if they could cause their cancer patients to experience an increase in a sense of well-being and appetite, a gain in weight, and especially a decrease in pain.
In the 1970’s, there was little chance that Laetrile would be given a chance to be tested except by its opponents. Every time proponents attempted to obtain permission to do so, they were turned down cold. On April 6, 1970, for example, the McNaughton Foundation, under the sponsorship of Andrew McNaughtonm submitted an application to the FDA for permission to engage in what is called IND (Investigation of New Drug) Phase One studies. Permission was granted on April 27. Then, in the words of one reporter, “All hell broke loose.”[24] The FDA apparently received a phone call from an irate and politically influential figure who passed the word: “Stop the tests!”
The next day, April 28, the FDA sent another letter to the Foundation advising that, upon reviewing the records, certain “deficiencies” had been found in the IND application, and demanding extensive additional data within ten days. Curiously, the letter was not delivered to the McNaughton Foundation until May 6, nine days after it supposedly had been written, and it is suspected that the letter may actually have been written much later but back-dated so as to make it impossible to comply with the already ridiculous ten day deadline. On May 12, six days after receipt of the “deficiency letter,” McNaughton received a telegram from the FDA advising him that the approval for the Investigation of New Drug had been revoked.
Nevertheless, hoping the FDA would reinstate its IND approval upon receipt of the additional data, McNaughton proceeded with the paperwork and, on May 15, just nine days after receipt of the FDA’s initial order, sent off to Washington everything that had been requested. By now, however, the FDA was firm. Laetrile would not be tested.
A former high official of the FDA told Dr. Dean Burk of the National Cancer Institute that he could not recall in over thirty years of service any instance in which just ten short days were demanded for a fifty page reply to alleged deficiencies. And, on Octover 1, 1970, there was nothing in the FDA procedural manual requiring termination notices after allowing only ten days for compliance.[25] Clearly, the entire action was contrived in response to political pressures as an excuse to stop the testing of Laetrile.
One of the reasons given for revoking approval for IND was that Laetrile might be toxic.
The FDA said solemnly:
Although it is often stated in the IND that amygdalin is non-toxic, data to demonstrate this lack of toxicity are absent… It is considered to be dangerous to base the starting dose for a chronic (6 + weeks) study in man on a single dose study in mice. It is also dangerous to initiate human studies while the nature of the toxicity has not been elucidated in large animal species.[26]
This is an incredible statement. First of all, as will be illustrated in a leter chapter, the non-toxicity of amygdalin (Laetrile) has been w well-known, fully accepted, and non-controversial fact for a hundred years. Second, the case histories submitted as part of the IND application were further proof of Laetrile’s safety. And third, the very question of toxicity is absurd inasmuch as all of the drugs approved by the FDA and currently used in orthodox cancer therapy are extremely toxic. To deny the testing of Laetrile on the grounds that it might be toxic is the height of sophistry.
Another reason given by the FDA for refusing to permit the testing of Laetrile was that the doctors who had used it did not keep sufficiently detailed clinical records. This, too, was a lame excuse, because Phase One studies do not require clinical records.
In righteous indignation, the courageous Dr. Burk of the National Cancer Institute wrote to Elliot Richardson, then Secretary of HEW (which administered the FDA), and said:
The granting of FDA permission for Phase One studies of IND has no absolute or invariable requirements for any clinical studies at all, although the sponsor is requested to supply any type of indication that he may posses, which the McNaughton Foundation has complied with to the limit of current feasibility. Dr. Contreras [of Mexico] and Dr. Nieper [of Germany] have been primarily preoccupied, quite justifiably, with treating cancer patients with Laetrile and related adjunctive therapies, and not with carrying out a clinical evolution of Laetrile in the precise and complete schedule of FDA protocols. For you to indicate that their records are inadequatre for such a purpose is clearly a red herring, since there is no such IND Phase One requirement involved, nor corresponding claim made.[25]
But the “fix” was on. Laetrile would not be approved for testing, regardless of the facts. On September 1, 1971, the FDA announced that the Ad Hoc Committee of Consultants for Review and Evaluation of Laetrile had found “no acceptable evidence of therapeutic effect to justify clinical trials.” And then it announced that, because of their findings, Laetrile could no longer be promoted, sold, or even tested in the United States.[27]
The California Report has remained as one of the primary authorities cited by cancer “experts” ad nauseum and as the basis of legal restraints against Laetrile. The cancer industry has also refused the advocates of Laetrile a chance to conduct their own clinical trials on the basis of such flimsy excuses that they would be laughable if the consequences were not so serious. All of this is the product of bias, not objectivity. The reports and pronouncements are calculated to deceive, not to clarify. It is fiat, not science.
Why is this happening? We shall deal with that part of the story next.
[1] “Debate Over Laetrile,” Time, April 12, 1971, p.20.
[2] "Laetrile Tiff, State Medic Out", San Jose Mercury (Calif), April 10, 1974
[3] Omar Garrison, The Dictocrats p. 130
[4] See Subcommittee on Health of the Committee on Labor and Public Welfare, Preclinical and Clinical Testing by the Pharmaceutical Industry, 1976, U.S. Sentate, Washington, D.C., 1976 pt.II, p.157.
[5] U.S. Senate, Competitive Problems in the Pharmaceutical Industry, 1969, pts. 6, 7 &10; cited by John Braithwaite, Corporate Crime in the Pharmaceutical Industry (London: Routledge & Kegan Paul, 1984), p. 52.
[6] Ibid.
[7] Braitwaite, op. cit. p. 53.
[8] Science.1973, vol. 180, p. 1038.
[9] Braitwaite, op. cit. p. 82.
[10] Arabella Melville and Colin Johnson, Cured to Death; The Effects of Prescription Drugs (New York: Stein & Day, 1982), p. 119.
[11] Braitwaite, op. cit. p. 82.
[12] Garrison, op. cit., pp. 134-35.
[13] Ibid., pp. 278-88.
[15] “Government is Suppressing Cancer Control, “ The National Tattler, March 11, 1973, p. 2.
[16] Cancer News Journal, January/April, 1971, p.22.
[17] “Here’s Another View: Tobacco May be Harmless,” U.S. News & World Report, Aug. 2, 1957, pp. 85-86.
[18] Third Research Conference, Committee for Research on Tobacco and Health, AMA Education and Research Foundation, May 7-9, 1972, p.4.
[19] See The Immoral Banning of Vitamin B-17, by Stewart M. Jones, M.S., M.D., Palo Alto, Calif., Jan., 1974, p.1. Also Cancer News Journal, Jan./April, 1971, p.3.
[20] Report by Cancer Advisory Council on Treatment of Cancer with Beta-Cyanogenic Glucosides (“Laetriles”), California Department of Public Health, 1963, Appendix 4 pp.1-2.
[21] Ibid., Appendix 3, pp.1-2.
[22] Report by Cancer Advisory Council, op. cit., p. 324.
[23] Current Diagnosis & Treatment, (Palo Alto:Lange Med. Publications, 1972), p. 902.
[24] Don C. Matchan, “Why Won’t They Test Laetrile?” Prevention, Jan., 1971, pp.149-150
[25] Letter from Dr. Dean Burk to Elliot Richardson, Secretary of HEW, dated Oct. 19, 1971; G. Edward Griffin, ed., Private Papers Relating to Laetrile, (Westlake Village, CA: American Media, 1997).
[26] The Ad Hoc Committee of Oncology Consultants For Review and Evaluation of Amygalin (Laetrile), FDA, Aug. 12, 1961, pp. 3-4.
[27] Press release, HFW/FDA, Sept. 1, 1971.
[5] U.S. Senate, Competitive Problems in the Pharmaceutical Industry, 1969, pts. 6, 7 &10; cited by John Braithwaite, Corporate Crime in the Pharmaceutical Industry (London: Routledge & Kegan Paul, 1984), p. 52.
[6] Ibid.
[7] Braitwaite, op. cit. p. 53.
[8] Science.1973, vol. 180, p. 1038.
[9] Braitwaite, op. cit. p. 82.
[10] Arabella Melville and Colin Johnson, Cured to Death; The Effects of Prescription Drugs (New York: Stein & Day, 1982), p. 119.
[11] Braitwaite, op. cit. p. 82.
[12] Garrison, op. cit., pp. 134-35.
[13] Ibid., pp. 278-88.
[15] “Government is Suppressing Cancer Control, “ The National Tattler, March 11, 1973, p. 2.
[16] Cancer News Journal, January/April, 1971, p.22.
[17] “Here’s Another View: Tobacco May be Harmless,” U.S. News & World Report, Aug. 2, 1957, pp. 85-86.
[18] Third Research Conference, Committee for Research on Tobacco and Health, AMA Education and Research Foundation, May 7-9, 1972, p.4.
[19] See The Immoral Banning of Vitamin B-17, by Stewart M. Jones, M.S., M.D., Palo Alto, Calif., Jan., 1974, p.1. Also Cancer News Journal, Jan./April, 1971, p.3.
[20] Report by Cancer Advisory Council on Treatment of Cancer with Beta-Cyanogenic Glucosides (“Laetriles”), California Department of Public Health, 1963, Appendix 4 pp.1-2.
[21] Ibid., Appendix 3, pp.1-2.
[22] Report by Cancer Advisory Council, op. cit., p. 324.
[23] Current Diagnosis & Treatment, (Palo Alto:Lange Med. Publications, 1972), p. 902.
[24] Don C. Matchan, “Why Won’t They Test Laetrile?” Prevention, Jan., 1971, pp.149-150
[25] Letter from Dr. Dean Burk to Elliot Richardson, Secretary of HEW, dated Oct. 19, 1971; G. Edward Griffin, ed., Private Papers Relating to Laetrile, (Westlake Village, CA: American Media, 1997).
[26] The Ad Hoc Committee of Oncology Consultants For Review and Evaluation of Amygalin (Laetrile), FDA, Aug. 12, 1961, pp. 3-4.
[27] Press release, HFW/FDA, Sept. 1, 1971.
========================
(Book World without Cancer - Chapter 8 )
“Laetrile is goddamned quackery!”The names, professional standings, medical achievements, and clinical findings of some of the more prominent doctors who endorse Laetrile; the beneficial side-effects produced by its use; a suggested anti-cancer diet; and a brief description of vitamin B15.
Such was the pronouncement of Helene Brown, president of the American Cancer Society of California. (1)
As early as 1974, there were at least twenty-six published papers written by well-known physicians who had used Laetrile in the treatment of their own patients and who have concluded (2) that Laetrile is both safe and effective in the treatment of cancer.
In addition, there are the voluminous private records of physicians who have used it clinically but have never published their findings except in letters to their colleagues or in public lectures or interviews. The American Cancer Society and other spokesmen. for orthodox medicine would have us believe that only quacks and crackpots have endorsed this conclusion. But the doctors who conducted these experiments and those who share their conclusions are not quacks. Here are just a few of the names:
1. “The Pain Exploiters; The Victimizing of Desperate Cancer Patients,” Today’s Health, Nov., 1973, p. 28.
2. A complete list of these papers is contained in The Laetriles/Nitrilosides, op. cit., pp. 84, 85.
In West Germany there is Hans Nieper, M.D., former Director of the Department of Medicine at the Silbersee Hospital in Hanover. He is a pioneer in the medical use of cobalt and is credited with developing the anti-cancer drug, cyclophosphamide. He is the originator of the concept of “electrolyte carriers” in the prevention of cardiac necrosis. He was formerly the head of the Aschaffenburg Hospital Laboratory for chemical circulatory research. He is listed in Who’s Who in World Science and has been the Director of the German Society for Medical Tumor Treatment. He is one of the world’s most famous and respected cancer specialists. During a visit to the United States in 1972, Dr. Nieper told news reporters:
After more than twenty years of such specialized work, I have found the nontoxic Nitrilosides—that is, Laetrile—far superior to any other known cancer treatment or preventative. In my opinion it is the only existing possibility for the ultimate control of cancer.In Canada there is N.R. Bouziane, M.D., former Director of Research Laboratories at St. Jeanne d’Arc Hospital in Montreal and a member of the hospital’s tumor board in charge of chemotherapy. He graduated magna cum laude in medicine from the University of Montreal. He also received a doctorate in science from the University of Montreal and St. Joseph’s Univer-sity, an affiliate of Oxford University in New Brunswick. He was a Fellow in chemistry and a Fellow in hematology, and certified in clinical bacteriology, hematology and biochemistry from the college. He also was Dean of the American Association of Bio-Analysts.
After the first series of tests with Laetrile shortly after it was introduced, Dr. Bouziane reported:
We always have a diagnosis based on histology [microscopic analysis of the tissue]. We have never undertaken a case without histological proof of cancer.... In our investigation, some terminal cases were so hopeless that they did not even receive what we consider the basic dose of thirty grams. Most cases, however, became ambulatory and some have in this short time resumed their normal activities on a maintenance dose.(1)1. “The Laetrile Story,” op. cit. p. 3. Also Cancer News Journal, Jan./Apr., 1971, p. 20.
In the Philippines there is Manuel Navarro, M.D., former Professor of Medicine and Surgery at the University of Santo Tomas in Manila; an Associate Member of the National Research Council of the Philippines; a Fellow of the Philippine College of Physicians, the Philippine Society of Endocrinology and Metabolism; and a member of the Philippine Medical Association, the Philippine Cancer Society, and many other medical groups. He has been recognized internationally as a cancer researcher and has over one-hundred major scientific papers to his credit, some of which have been read before the International Cancer Congress. In 1971 Dr. Navarro wrote:
I ... have specialized in oncology [the study of tumors] for the past eighteen years. For the same number of years I have been using Laetrile—amygdalin in the treatment of my cancer patients. During this eighteen year period I have treated a total of over five hundred patients with Laetrile—amygdalin by various routes of administra-tion, including the oral and the I.V. The majority of my patients receiving Laetrile—amygdalin have been in a terminal state when treatment with this material commenced.1. Letter from Dr. Navarro to Mr. Andrew McNaughton, The McNaughton Foundation, dated January 8, 1971, published in the Cancer News Journal, Jan/April, 1971. pp. 19. 20.
It is my carefully considered clinical judgment, as a practicing oncologist and researcher in this field, that I have obtained most significant and encouraging results with the use of Laetrile—amygdalin in the treatment of terminal cancer patients, and that these results are comparable or superior to the results I have obtained with the use of the more toxic standard cytotoxic agents.
In Mexico there is Ernesto Contreras, M.D., who, for over three decades, has operated the Good Samaritan Cancer Clinic (now called the Oasis Hospital) in Tijuana. He is one of Mexico’s most distinguished medical figures. He received postgraduate training at Harvard’s Children’s Hospital in Boston. He has served as Professor of Histology and Pathology at the Mexican Army Medical School and as the chief pathologist at the Army Hospital in Mexico City.
Dr. Contreras was introduced to Laetrile in 1963 by a terminal cancer patient from the United States who brought it to his. attention and urged him to treat her with it. The woman recovered, and Dr. Contreras began extensive investigation of its properties and use. Since that time he has treated many thousands of cancer patients, most of whom are American citizens who have been denied the freedom to use Laetrile in their own country Dr. Contreras has summarized his experiences with vitamin therapy as follows:
The palliative action [improving the comfort and well-being of the patient] is in about 60% of the cases. Frequently, enough to be significant, I see arrest of the disease or even regression in some 15% of the very advanced cases. (1)1. Cancer News Journal, Jan. /April, 1971, p. 20. We must bear in mind that these are terminal patients—people who have been given up as hopeless by orthodox medicine. Fifteen percent recovery in that group is a most impressive accomplishment.
In Japan there is Shigeaki Sakai, a prominent physician in Tokyo. In a paper published in the October 1963 Asian Medical Journal, Dr. Sakai reported:
Administered to cancer patients, Laetrile has proven to be quite free from any harmful side-effects, and I would say that no anti-cancer drug could make a cancerous patient improve faster than Laetrile. It goes without saying that Laetrile controls cancer and is quite effective wherever it is located.In Italy there is Professor Etore Guidetti, M.D., of the University of Turin Medical School. Dr. Guidetti spoke before the Conference of the International Union Against Cancer held in Brazil in 1954 and revealed how his use of Laetrile in terminal cancer patients had caused the destruction of a wide variety of tumors including those of the uterus, cervix, rectum, and breast. “In some cases,” he said, “one has been able to observe a group of fulminating and cauliflower-like neoplastic masses resolved very rapidly” He reported that, after giving Laetrile to patients with lung cancer, he had been “able to observe, with the aid of radiography, a regression of the neoplasm or the metastases.”
After Guidetti’s presentation, an American doctor rose in the audience and announced that Laetrile had been investigated in the United States and found to be worthless. Dr. Guidetti replied, “I do not care what was determined in the United States. I am merely reporting what I saw in my own clinic.”(2)
2. Cancer News Journal, Jan/April, 1971, p. 19.
In Belgium there is Professor Joseph H. Maisin, Sr., M.D., of the University of Louvain where he was Director of the Institute of Cancer. He also was President Emeritus of the International League Against Cancer which conducts the International Cancer Congress every four years.
And in the United States there are such respected names as Dr. Dean Burk of the National Cancer Institute; Dr. John A. Morrone of the Jersey City Medical Center; Dr. Ernst T. Krebs, Jr., who developed Laetrile; Dr. John A. Richardson, the courageous San Francisco physician who challenged the government’s right to prevent Laetrile from being used in the United States; (1) Dr. Philip E. Binzel,, Jr., a physician in Washington Court House, Ohio, who has used Laetrile for over twenty years with outstanding success; and many others from over twenty countries with equally impeccable credentials.
Most of these practitioners have reported independently that patients usually experience several important side effects. These include a normalizing of blood pressure in hypertensive patients, improved appetite, an increase in the hemoglobin and red blood cell count, the elimination of the fetor (which is the unpleasant odor often associated with terminal cancer patients), and above all, a release from pain without narcotics. Even if the patient has started Laetrile therapy too late to be saved, this last effect is a merciful blessing in itself.
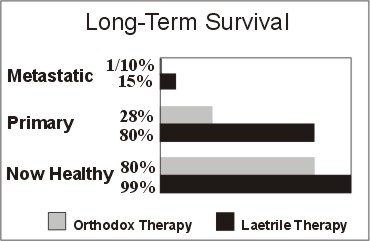
One must not conclude that the only value in Laetrile is to improve the quality of life as the patient is dying. Extension of the length of life is the grand prize for many patients. Dr. Binzel, in his book, Alive and Well, compared the long-term survival statistics of his own cancer patients with the survival rates of those who undergo orthodox therapies. His study involved 108 patients representing 23 different types of cancer. This is what he reported:
This means that out of 108 patients with metastatic cancer, over a period of 18 years, 76 of those patients (70.4%) did not die of their disease. Again, even if I concede that the 9 patients who died of “cause unknown” did, indeed, die from their cancer, I am looking at 62.1% [long-term survival]....1. See John A. Richardson, M.D., and Patricia Griffin, R.N., Laetrile Case Histories; The Richardson Cancer Clinic Experience (Westlake Village, CA: American Media, 1977).
If you consider only those patients who have survived five years or more, this means that my results were 287% better than those reported by the American Cancer Society for the treatment of metastatic cancer by “orthodox” methods alone.(2)
2. Philip E. Binzel, M.D., Alive and Well: One Doctor’s Experience with Nutrition in the Treatment of Cancer Patients (Westlake Village, CA: American Media, 1994), p. 113.
The following graph, taken from Dr. Binzel’s book, Alive and Well, shows his comparison between nutritional and conventional therapies. Primary Cancer represents patients with only one cancer location. Metastatic Cancer represents patients whose cancer has spread to multiple locations.
 In addition to the clinical results obtained by these physicians in the treatment of humans, there have been at least five carefully controlled experiments on mice that have shown definite Laetrile anti-cancer action. These include: (1) the experiments done by Scind Laboratories of San Francisco in 1968, (2) the studies completed at the Pasteur Institute (Paris) in 1971, (3) those at the Institute von Ardenne (Dresden, Germany) in 1973, (4) the experiments at the Southern Research Institute in 1973, and (5) numerous trials at Sloan-Kettering from 1972 to 1977. In spite of all this, spokesmen for orthodox medicine still proclaim there is no evidence that Laetrile works. The evidence is everywhere.(1)
In addition to the clinical results obtained by these physicians in the treatment of humans, there have been at least five carefully controlled experiments on mice that have shown definite Laetrile anti-cancer action. These include: (1) the experiments done by Scind Laboratories of San Francisco in 1968, (2) the studies completed at the Pasteur Institute (Paris) in 1971, (3) those at the Institute von Ardenne (Dresden, Germany) in 1973, (4) the experiments at the Southern Research Institute in 1973, and (5) numerous trials at Sloan-Kettering from 1972 to 1977. In spite of all this, spokesmen for orthodox medicine still proclaim there is no evidence that Laetrile works. The evidence is everywhere.(1)1. "See How They Lie, See How They Lie" By Dr. Dean Burk, Cancer News Journal, Vol. 9, No. 3 (June, 1974), p. 5.
While the use of Laetrile alone has proven to be effective in many instances, even better results usually are obtained with supplemental therapy as well. The late John Richardson, M.D., of San Francisco achieved one of the highest recovery rates among Laetrile practitioners in the entire world. Here, in his own words, is the advice he gave to his patients:
Vegetable Kingdom: In the vegetable kingdom eat anything and everything that is edible and for which you have no idiosyncrasy Eat everything whole. Eat all of the edible parts of the food— especially the roughage. This food is preferably eaten raw; but when you cannot tolerate it raw, cook the food just sufficiently to make it tolerable.The dietary restrictions prescribed by Dr. Richardson are for those who have cancer. It is not recommended for healthy persons because it is unnecessarily restrictive. For those who do not have cancer, a general diet containing foods rich in nitriloside content (2) should be adequate. Here is what Dr. Krebs suggests:
Animal Kingdom: Eat any or all fish as fresh as possible and lightly cooked in the absence of animal fats (vegetable oils may be used). Eat the skin-free meat of poultry. Whatever does not fall within this formula, forget it. Don’t eat it. The formula is all-inclusive, so it’s not necessary to mention: no dairy products, beef, mutton, pork, bacon, ham, etc. The liver is to neoplastic diseases what the heart is to circulatory diseases. The liver is central.
Adequate liquid intake with fresh juices plain or carbonated.
Vitamin Supplements: Vit. C, 1500 mg to 5000 mg; 800 — 1200 International Units of d-alpha tocopherol (vitamin E) plus a good brand of therapeutic multi-vitamins, preferably of organic or natural derivatives. Toxins of all kinds to be avoided including, tobacco, alcohol. Discourage coffee, tranquilizers, sedatives, analgesics. Antibiotics OK. Rest is important while exercise should spare the affected area......
You should include Vitamin B15 (pangamic acid) which detoxifies the liver as a transmethylating agent, and increases the oxygen uptake potential of the tissues, and since trophoblast lives by the fermentative process, the rationale for the B15 is obvious. Pancreatic Enzyme Supplementation: We find dessicated pancreas substances to be an effective supplement.(1)
1. Open letter to interested doctors dated Nov. 1972, revised 1974; Griffin, Private Papers, op. cit.
2. Again, we highly recommend June de Spain’s The Little Cyanide Cookbook, op. cit.
For breakfast, gruel of buckwheat, millet, and flaxseed, with elderberry jelly on millet toast. All this accompanied by stewed prunes.Dr. Krebs has pointed out that in the Old Testament there is a formula for the preparation of grains for bread, and it speaks of six ingredients, five of which are rich in nitrilosides. They are barley, beans, lentils, millet and vetch (chickpea or garbanzo beans).(1)
For lunch, lima beans or a succotash with chick peas; millet rolls with plum jam; elderberry wine.
For dinner, a salad with bean and millet sprouts; dinner rolls of buckwheat and millet sweetened with sorghum molasses extracted from sorghum cane; rabbit which, hopefully, fed on clover; and after dinner apricot, peach, cherry, or plum brandy originally prepared from crushing the entire or whole fruit.
Nibbling on any member of the raspberry family, macadamia nuts, and bamboo sprouts is also suggested.
1. Ezekiel IV: 9
The intended balance of nature does not require a vast amount of vitamin B17 in the daily diet any more than it is required of the other vitamins. It is possible that if one did no more than eat the seeds from an apple or two a day he could obtain an adequate supply. But that would probably be bordering on the low side, especially considering that, in westernized society, B17 is not generally available in other foods to supplement it. So it probably would be advisable to obtain a higher level of intake than that.
Obviously, some of the foods mentioned by Dr. Krebs are not readily available to the average city dweller. As a substitute, many people simply have adopted the habit of eating six to twelve apricot or peach seeds each day, or have ground them in their blenders and used them as a light seasoning for cereals, salads, and the like. For those who dislike the slight bitter taste of these seeds, they can be ground up and loaded into empty capsules. Which means that no one need be deprived of this vitamin if he really wants it.
Vitamin B15 has been mentioned several times as an important auxiliary therapy to vitamin B17, and there often is confusion between the two. So let’s take a moment to differentiate.
Vitamin B15 sometimes is called pangamic acid. Pan implies everywhere and gami means seed. It was so named because it is found in small amounts almost everywhere on earth in seeds and usually in the company of other members of the vitamin-B complex. Like B17, it too was discovered by Dr. E.T. Krebs, Jr., while exploring the chemical properties of apricot kernels in 1952. It could be said that it was an unexpected bonus or by-product of the search for vitamin B17.
The best way to understand the effect of vitamin B15 is to think of it as instant oxygen. It increases the oxygen efficiency of the entire body and aids in the detoxification of waste products. Since cancer cells do not thrive in the presence of oxygen but depend rather on fermentation of glucose, it is probable that B15, indirectly, is an enemy of cancer.
Vitamin B15 is not widely known or used in the United States. The reason is almost an exact parallel to the Laetrile story. The government officially has refused to recognize that B15 is of value. Meanwhile it is used extensively in many other countries. Russia in particular is far ahead of the United States in the use of this substance and has conducted extensive research into its uses. In fact, in 1965 the U.S.S.R. Academy of Sciences released a 205-page symposium of its findings up to that date. In 1968 the Scientific Advisory Committee of the Ministry of Health unanimously ratified all the original claims in the report and authorized the Soviet drug industry to begin mass-production of B15 for general use.
It has been reported that the Russian athletes have been given heavy doses of B15 during their participation at the Olympics. If this is true, there is good reason for it. Experiments have shown that this substance, although just a natural food factor, greatly increases physical strength and stamina. When rats were put into tubs of water and forced to swim, those that had been vitaminized with B15 were all still swimming long after the others had fatigued and drowned. When other rats were put into glass chambers from which oxygen gradually was removed, the vitaminized rats lived much longer—thus on less oxygen—than the control group.
The Soviet scientists disclosed that vitamin B15 is effective in such areas as circulatory problems, heart conditions, elevated blood cholesterol, skin disorders, hardening of the arteries, bronchial asthma, diabetes mellitus, and wound healing. They were especially emphatic in their findings that B15 was effective in retarding the aging process! Professor Shpirt of the City Clinical Hospital No. 60 in Moscow concluded: “I believe the time will come when there will be calcium pangamate (B15) next to the salt shaker on the table of every family with people past forty.”(1)
1. For a detailed analysis of these findings, see Vitamin B5 (Pangamic Acid); Properties, Functions, and Use. (Moscow: Science Publishing House, 1965), translated and reprinted by McNaughton Foundation, Sausalito, Calif.
Doctors who wish to use vitamin B15 in America have been forced to operate on the fringe of the law because their government has harassed its manufacturers and blocked its movement in commerce. As Dr. Krebs observed:
Our concern is with vitamin B15—a natural constituent of natural foods, one that experimentation has shown to be of definite value in increasing resistance to disease and in maintaining healthy functioning of the body as well.Fortunately, there is some evidence that B15 is finally becoming recognized by several of the more prestigious medical institu-tions in spite of government obstacles. Let us hope that the trend rapidly continues.
Pangamic acid is giving the people of Russia, Japan, Yugoslavia, France, Spain, and Germany a tremendous health and longevity advantage. But it is not available to us in the land in which it was first discovered.
It is possible that B15 will be recognized and accepted by orthodox medicine long before B17. This is because there is less vested interest to overcome. There have been no broad deroga-tory pronouncements by the AMA and, hence, no reputations are at stake. But, in time, the sheer weight of the facts will force the acceptance of B17 as well. And the men who now bear the brunt of controversy, professional ostracism, and social scorn, will emerge, not as quacks, but as the great medical pioneers of their day.
======================
The Hoax Of The "Proven" Cancer Cures
Chapter 10 from World Without Cancer by Edward Griffin
The advocates of Laetrile therapy have always emphasized that there is no cure, as such, for cancer. Since it is essentially a deficiency disease, one can only speak of prevention or control but not cure. Among the advocates of orthodox therapies, however, there is no such restraint. Official spokesmen for the cancer industry tell the American public, without batting an eyelash, that they have proven cures for cancer, and that anyone who resorts to such nostrums as Laetrile is merely wasting valuable time in which he would be far better off availing himself of these proven cures. What are these cures? They are surgery, radiation, and drugs. The following report carried in a Los Angeles paper is typical:The effects of surgery and radiation in the treatment of cancer; a comparison showing that those who receive no treatment at all live just as long, if not longer, than those who are treated.
Warnings of a mounting scale of cancer quackery activity affecting the San Fernando Valley were issued today by the American Cancer Society.Echoing the same theme, Dr. Ralph Weilerstein of the California Department of Public Health declared:
Mrs. Stanley Grushesky, Education Chairman of the Society's Valley area, said she is concerned over the possibility that some local residents have been deceived in recent weeks by propaganda issued on behalf of unorthodox practitioners with claims of unproven cancer cures.
She declared that "under the banners of freedom of speech, with the slogan of freedom of choice, advocates of unorthodox cancer remedies have been making wild claims which could easily lure unsuspecting victims into a quackery mill."...
Mrs. Grushesky said that surgery and radiation are the only known methods for successfully treating cancer, although some beneficial effects have been obtained in certain cases through the administration of chemicals or hormones....
"Cancer quackery kills many unsuspecting patients because time wasted on phony devices and treatments delays effective treatment until it is too late to save the patient's life."1
The use of Laetrile in early cancer cases to the exclusion of conventional treatment might well be dangerous since treatment with acceptable, modern curative methods-surgery or radiation-would thereby be delayed potentially until such time as metastases had occurred and the cancer, therefore, might no longer be curable.2Public Library reference volumes on cancer often contain bookmarks distributed by the American Cancer Society. One of these depicts an ace of spades along with the slogan: THE UNPROVEN CANCER CURE. DON'T BET YOUR LIFE ON IT. On the back it says: "For more information on proven cancer cures, write or phone the American Cancer Society." In response, the author sent a letter to the ACS headquarters expressing surprise at the assertion that there is any cancer therapy successful enough to warrant being called a proven cure. This is the reply received:
To Mr. G. Edward Griffin:
Thank you for your note. There are proven cures - if detected in time-surgery and/or radiation and, more and more, chemotherapy is playing its part.3
This, then, is the position of orthodox medicine. Therefore, let us take a look at the results and benefits of the so-called cures obtained through surgery, radiation, and chemotherapy. Surgery is the least harmful of the three. In some cases, it can be a life-saving, stop-gap measure-particularly where intestinal blockages must be relieved to prevent immediate death from secondary complications. Surgery also has the psychological advantage of visibly removing the tumor. From that point of view, it offers the temporary comfort and hope. However, the degree to which surgery is useful is the same degree to which the tumor is not malignant, The greater the proportion of cancer cells in that tumor, the less likely it is that surgery will help. The most highly malignant tumors of all generally are considered inoperable.
A further complication of surgery is the fact that cutting into the tumor-even for a biopsy-does two things that aggravate the condition. First, it causes physical trauma to the area. This triggers off the healing process which, in turn, brings more trophoblast cells into being as a by-product of that process. (See Chapter IV.) The other effect is that, if not all the malignant tissue is removed, what remains tends to be encased in scar tissue from the surgery Scar tissue tends to act as a barrier between the cancer cell and the rest of the body Consequently, the cancer tends to become insulated from the action of the pancreatic enzymes which, as we have seen, are so essential in exposing trophoblast cells to the surveillant action of the white blood cells.
Perhaps the greatest indictment of all against surgery is the gnawing suspicion among even many of the world's top surgeons that, statistically, there is no solid evidence that patients who submit to surgery have any greater life expectancy, on the average, than those who do not. This is an area which desperately needs intensive and unbiased study The first statistical analysis of this question was compiled in 1844 by Dr. Leroy d'Etoilles and published by the French Academy of Science. It is, to date, the most extensive study of its kind ever released. Over a period of thirty years, case histories of 2,781 patients were submitted by 174 physicians. The average survival after surgery was only one year and five months-not much different than the average today.
Dr. Leroy d'Etoilles separated his statistics according to whether the patient submitted to surgery or caustics, or refused such treatment. His findings were electric:
1844 was a long time ago, but more recent surveys have produced nearly the same results. For example, it long has been accepted practice for patients with breast cancer to have not only the tumor removed but the entire breast and the lymph nodes as well. The procedure sometimes included removal of the ovaries also on the theory that cancer is stimulated by their hormones. Finally, in 1961, a large-scale controlled test was begun, called the National Surgical Adjuvant Breast Project. After seven-and-a-half years of statistical analysis, the results were conclusive: There was no significant difference between the percentage of patients remaining alive who had received the smaller operation and those who had received the larger.5The net value of surgery or caustics was in prolonging life two months for men and six months for women. But that was only in the first few years after the initial diagnosis. After that period, those who had not accepted treatment had the greater survival potential by about fifty percent.4
A similar study conducted between 1984 and 1990 at the University of California-Irvine College of Medicine produced the same conclusion: "All other factors being equal, there is no difference between BCS [breast-conserving surgery] and total mastectomy in either disease-free or overall survival."6
One of the nation's top statisticians in the field of cancer is Hardin B. Jones, Ph.D., former professor of medical physics and physiology at the University of California at Berkeley. After years of analyzing clinical records, this is the report he delivered at a convention of the American Cancer Society:
In regard to surgery, no relationship between intensity of surgical treatment and duration of survival has been found in verified malignancies. On the contrary, simple excision of cancers has produced essentially the same survival as radical excision and dissection of the lymphatic drainage.7 That data, of course, related to surgery of the breast.Turning his attention to surgery in general, Dr. Jones continued:
Although there is a dearth of untreated cases for statistical comparison with the treated, it is surprising that the death risks of the two groups remain so similar. In the comparisons it has been assumed that the treated and untreated cases are independent of each other. In fact, that assumption is incorrect. Initially, all cases are untreated. With the passage of time, some receive treatment, and the likelihood of treatment increases with the length of time since origin of the disease. Thus, those cases in which the neoplastic process progresses slowly [and thus automatically favors a long-term survival] are more likely to become "treated" cases. For the same reason, however, those individuals are likely to enjoy longer survival, whether treated or not. Life tables truly representative of untreated cancer patients must be adjusted for the fact that the inherently longer-lived cases are more likely to be transferred to the "treated" category than to remain in the "untreated until death."What, then, is the statistical chance for long-term survival of five years or more after surgery? That, we are told, depends on the location of the cancer, how fast it is growing, and whether it has spread to a secondary point. For example, two of the most common forms of cancer requiring surgery are of the breast and the lung. With breast cancer, only sixteen percent will respond favorably to surgery or X-ray therapy With lung cancer, the percentage of patients who will survive five years after surgery is somewhere between five and ten percent.8 And these are optimistic figures when compared to survival expectations for some other types of cancers such as testicular chorionepitheliomas. When we turn to cancers which have metastasized to secondary locations, the picture becomes virtually hopeless-surgery or no surgery As one cancer specialist summarized it bluntly:
The apparent life expectancy of untreated cases of cancer after such adjustment in the table seems to be greater than that of the treated cases. [Emphasis added]
A patient who has clinically detectable distant metastases when first seen has virtually a hopeless prognosis, as do patients who were apparently free of distant metastases at that time but who subsequently return with distant metastases.9An objective appraisal, therefore, is that the statistical rate of long-term survival after surgery is, on the average at best, only ten or fifteen percent. And once the cancer has metastasized to a second location, surgery has almost no survival value. The reason is that, like the other therapies approved by orthodox medicine, surgery removes only the tumor. It does not remove the cause.
The rationale behind X-ray therapy is the same as with surgery. The objective is to remove the tumor, but to do so by burning it away rather than cutting it out. Here, also, it is primarily the non-cancer cell that is destroyed. The more malig-nant the tumor, the more resistant it is to radio therapy If this were not so, then X-ray therapy would have a high degree of success-which, of course, it does not.
If the average tumor is composed of both cancer and non-cancer cells, and if radiation is more destructive to non-cancer cells than to cancer cells, then it would be logical to expect the results to be a reductionof tumor size, but also an increase in the percentage of malignancy. This is, in fact, exactly what happens. Commenting on this mechanism, Dr. John Richardson explained it this way:
Radiation and/or radiomimetic poisons will reduce palpable, gross or measurable tumefaction. Often this reduction may amount to seventy-five percent or more of the mass of the growth. These agents have a selective effect-radiation and poisons. They selectively kill everything except the definitively neoplastic [cancer] cells.And so we see that X-ray therapy is cursed with the same drawbacks of surgery. But it has one more: It actually increases the likelihood that cancer will develop in other parts of the body!
For example, a benign uterine myoma will usually melt away under radiation like snow in the sun. If there be neoplastic cells in such tumor, these will remain. The size of the tumor may thus be decreased by ninety percent while the relative concentration of definitively neoplastic cells is thereby increased by ninety percent.
As all experienced clinicians know-or at least should know- after radiation or poisons have reduced the gross tumefaction of the lesion the patient's general well-being does not substantially im-prove. To the contrary, there is often an explosive or fulminating increase in the biological malignancy of his lesion. This is marked by the appearance of diffuse metastasis and a rapid deterioration in general vitality followed shortly by death.10
Excessive exposure to radioactivity is an effective way to induce cancer. This was first demonstrated by observing the increased cancer incidence among the survivors of Hiroshima, but it has been corroborated by many independent studies since then. For example, a recent headline in a national-circulation newspaper tells us: FIND 'ALARMING' NUMBER OF CANCER CASES IN PEOPLE WHO HAD X-RAY THERAPY 20 YEARS AGO.11
The Textbook of Medical Surgical Nursing, a standard reference for Registered Nurses, is most emphatic on this point. It says:
This is an area of public health concern because it may involve large numbers of people who may be exposed to low levels of radiation over a long period of time. The classic example is of the women employed in the early 1920's to paint watch and clock dials with luminizing (radium containing) paints. Years later, bone sarcomas resulted from the carcinogenic effect of the radium. Similarly, leukemia occurs more frequently in radiologists than other physicians. Another example is the Hiroshima survivors who have shown the effects of low levels of radiation....In 1971, a research team at the University of Buffalo, under the direction of Dr. Robert W. Gibson, reported that less than a dozen routine medical X-rays to the same part of the body increases the12 risk of leukemia in males by at least sixty percent. Other scientists have become increasingly concerned about the growing American infatuation with X-rays and have urged a stop to the madness, even calling for an end to the mobile chest X-ray units for the detection of TB.13 And these "routine" X-rays are harm-lessly mild compared to the intense radiation beamed into the bodies of cancer patients today.
Among the most serious of the late consequences of irradiation damage is the increased susceptibility to malignant metaplasia and the development of cancer at sites of earlier irradiation. Evidence cited in support of this relationship refers to the increased incidence of carcinoma of skin, bone, and lung after latent periods of 20 years and longer following irradiation of those sites. Further support has been adduced from the relatively high incidence of carcinoma of the thyroid 7 years and longer following low-dosage irradiation of the thymus in childhood, and from the increased incidence of leukemia following total body irradiation at any age.
X-rays induce cancer because of at least two factors. First, they do physical damage to the body which triggers the production of trophoblast cells as part of the healing process. Second, they weaken or destroy the production of white blood cells which, as we have seen, constitute the immunological defense mechanism, the body's front-line defense against cancer.
Now to the question of statistics. Again we find that, on the average, there is little or no solid evidence that radiation actually improves the patient's chances for survival. The National Surgical Adjuvant Breast Project, previously mentioned in connection with surgery, also conducted studies on the effect of irradiation, and here is a summary of their findings:
From the data available it would seem that the use of post-operative irradiation has provided no discernible advantage to patients so treated in terms of increasing the proportion who were free of disease for as long as five years.14This is an embarrassingly difficult fact for a radiologist to face, for it means, quite literally, that there is little justification for his existence in the medical fraternity. If he were to admit publicly what he knows privately, a guy could talk himself right out of a job! Consequently, one does not expect to hear these facts being discussed by radiologists or those whose livelihood depends on the construction, sale, installation, use, or maintenance of the multi-million-dollar linear accelerators. It comes as a pleasant surprise, therefore, to hear these truths spoken frankly and openly by three well known radiologists sharing the same platform at the same medical convention. They were William Powers, M.D., Director of the Division of Radiation Therapy at the Washington University School of Medicine, Phillip Rubin, M.D., Chief of the Division of Radiotherapy at the University of Rochester Medical School, and Vera Peters, M.D., of the Princess Margaret Hospital in Toronto, Canada. Dr. Powers stated:
Although preoperative and postoperative radiation therapy have been used extensively and for decades, it is still not possible to prove unequivocal clinical benefit from this combined treatment.... Even if the rate of cure does improve with a combination of radiation and therapy, it is necessary to establish the cost in increased morbidity which may occur in patients without favorable response to the additional therapy.15What Dr. Powers means when he speaks of "increased morbidity" is that radiation treatments make people ill. In a study at Oxford University dealing with breast cancer, it was found that many women who received radiation died of heart attacks because their hearts had been weakened by the treatment.16 Radiation also weakens the immune system which can lead to death from secondary causes such as pneumonia or other internal infections. Many patients whose death certificates state heart failure or pulmonary pneumonia or respiratory failure really die from cancer-or, to be more exact-from their cancer treatment. This is another reason that cancer statistics-based as they are on data from death certificates-conceal the truth about the failure of orthodox cancer therapy
At the medical convention of radiologists previously mentioned, Dr. Phillip Rubin reviewed the cancer-survival statistics published in the Journal of the American Medical Association. Then he concluded:
The clinical evidence and statistical data in numerous reviews are cited to illustrate that no increase in survival has been achieved by the addition of irradiation.To which Dr. Peters added:
In carcinoma of the breast, the mortality rate still parallels the incidence rate, thus proving that there has been no true improvement in the successful treatment of the disease over the past thirty years, even though there has been technical improvement in both surgery and radiotherapy during that time.In spite of the almost universal experience of physicians to the contrary, the American Cancer Society still prattles to the public that their statistics show a higher recovery rate for treated patients as compared to untreated patients. After all, if this were not the case, why on earth would anyone spend the money or undergo the pain and disfigurement associated with these orthodox treatments? But how can they get away with such outright lies?
The answer is that they are not really lying-just bending the truth a little. In other words, they merely adjust the method of gathering and evaluating statistics so as to guarantee the desired results. In the words of Dr. Hardin Jones:
Evaluation of the clinical response of cancer to treatment by surgery and radiation, separately or in combination, leads to the following findings:But there is far more to it than that. Such statistical error is significant, but it is doubtful if it could account for the American Cancer Society's favorite claim that "there are on record a million and a half people cured of cancer through the efforts of the medical profession and the American Cancer Society with the help of the FDA."18
The evidence for greater survival of treated groups in compari-son with untreated is biased by the method of defining the groups. All reported studies pick up cases at the time of origin of the disease and follow them to death or end of the study interval. If persons in the untreated or central group die at any time in the study interval, they are reported as deaths in the control group. In the treated group, however, deaths which occur before completion of the treatment are rejected from the data, since these patients do not then meet the criteria established by definition of the term "treated." The longer it takes for completion of the treatment, as in multiple step therapy, for example, the worse the error.... With this effect stripped out, the common malignancies show a remarkably similar rate of demise, whether treated or untreated.17
The answer lies in the fact that there are some forms of cancer, such as skin cancer, that respond very well to treatment. In fact, often they are arrested or disappear even without treatment. Seldom are they fatal. But they affect large numbers of people- enough to change the statistical tabulations drastically. In the beginning, skin cancers were not included in the national tabulations. Also, in those days, very few people sought medical treatment for their skin disorders, preferring to treat them with home remedies, many of which, incidentally seem to have worked just as well as some of the more scientifically acceptable techniques today.
At any rate, as doctors became more plentiful, as people became more affluent and able to seek out professional medical help, and as the old-time remedies increasingly fell into disrepute, the number ofreported skin cancers gradually increased until it is now listed by the ACS as a "major site." So, all they had to do to produce most of those million-and-a-half "cures," was to change their statistics to include skin cancers-presto-chango!
As Dr. Hardin Jones revealed:
Beginning in 1940, through redefinition of terms, various questionable grades of malignancy were classed as cancer. After that date, the proportion of "cancer" cures having "normal" life expectancy increased rapidly, corresponding to the fraction of question-able diagnoses included.19The American Cancer Society claims that cancer patients are now surviving longer, thanks to orthodox therapy. In truth, however, people are not living longer after they get cancer; they are living longer after they are diagnosed with cancer. The trick is that, with modern diagnostic techniques, it is possible to identify cancer at an earlier stage than before. So the time between diagnosis and death is longer, but the length of life itself has not been increased at all.20 This is merely another statistical deception.
When X-ray therapy is used, the body's white blood cell count is reduced which leaves the patient susceptible to infections and other diseases as well. It is common for such patients to succumb to pneumonia, for instance, rather than cancer. And, as stated previously, that is what appears on the death certificate-as well as in the statistics. As Dr. Richardson has observed:
I have seen patients who have been paralyzed by cobalt spine radiation, and after vitamin treatment their HCG test is faintly positive. We got their cancer, but the radiogenic manipulation is such that they can't walk.... It's the cobalt that will kill, not the cancer.21If the patient is strong enough or lucky enough to survive the radiation, then he still faces a closed door. As with all forms of currently popular treatments, once the cancer has metastasized to a second location, there is practically no chance that the patient will live. So, in addition to an almost zero survival value, radio therapy has the extra distinction of also spreading the very cancer it is supposed to combat.
One of the most publicized claims by The American Cancer Society is that early diagnosis and treatment increases the chance of survival. This is one of those slogans that drives millions of people into their doctors' offices for that mystical experience called the annual checkup. "A check and a checkup" may be an effective stimulus for revenue to the cancer industry but its medical value is not as proven as the hype would suggest. As Dr. Hardin Jones stated emphatically:
In the matter of duration of malignant tumors before treatment, no studies have established the much talked about relationship between early detection and favorable survival after treatment.... Serious attempts to relate prompt treatment with chance of cure have been unsuccessful. In some types of cancer, the opposite of the expected association of short duration of symptoms with a high chance of being "cured" has been observed. A long duration of symptoms before treatment in a few cancers of the breast and cervix is associated with longer than usual survival.... Neither the timing nor the extent of treatment of the true malignancies has appreciably altered the average course of the disease. The possibility exists that treatment makes the average situation worse. 22In view of all this, it is exasperating to find spokesmen for orthodox medicine continually warning the public against using Laetrile on the grounds that it will prevent cancer patients from benefiting from "proven" cures. The pronouncement by Dr. Ralph Weilerstein of the California Department of Public Health cited at the opening of this chapter is typical. But Dr. Weilerstein is vulnerable on two points. First, it is very rare to find any patient seeking Laetrile therapy who hasn't already been subjected to the so-called "modern curative methods" of surgery and radiation. In fact, most of them have been pronounced hopeless after these methods have failed, and it is only then that these people turn to vitamin therapy as a last resort. So Dr. Weilerstein has set up a straw-man objection on that score. But, more important than that is the fact that the Weilersteinian treatments simply do not work.
Battling as a lone warrior within the enemy stronghold, Dr. Dean Burk of the National Cancer Institute repeatedly has laid it on the line. In a letter to his boss, Dr. Frank Rauscher, he said:
In spite of the foregoing evidence,.., officials of the American Cancer Society and even of the National Cancer Institute, have continued to set forth to the public that about one in every four cancer cases is now "cured" or "controlled," but seldom if ever backed up with the requisite statistical or epidemiological support for such a statement to be scientifically meaningful, however effective for fund gathering. Such a statement is highly misleading, since it hides the fact that, with systemic or metastatic cancers, the actual rate of control in terms of the conventional five-year survival is scarcely more than one in twenty..The statistics of the ACS are fascinating to study. They constitute page after page of detailed tables and complex charts telling about percentages of cancer by location, sex, age, and geography. But when it comes to hard numbers about their so-called "proven cures," there is nothing. The only "statistic" one can get is their unsupported statement: "One out of three patients is being saved today as against one out of five a generation ago." This may or may not be true, depending on one's definition of the word saved. But even if we do not challenge it, we must keep in mind that there also is a correspondingly larger gain in the number of those who are getting cancer. Why is that?
One may well ask Dr. Weilerstein where are all the modern curative methods to which he, the California Cancer Advisory Council, and indeed so many administrators so glibly refer?... No, disseminated cancer, in its various forms and kinds remains, by and large, as "incurable" as at the time of the Kefauver Amendment ten years ago-Dr. Weilerstein or no Dr. Weilerstein, FDA or no FDA, ACS or no ACS, AMA or no AMA, NCI or no NCI.23
Here is the official explanation:
Major factors are the increasing age and size of the population. Science has conquered many diseases, and the average life span of Americans has been extended. Longer life brings man to the age in which cancer most often strikes-from the fifth decade on.All of which sounds plausible-until one examines the facts: First, the increasing size of the population has nothing to do with it. The statistics of "one out of three" and "one out of five" are proportional rather than numerical. They represent ratios that apply regardless of the population size. They cannot explain the increasing cancer rate.
Second, the average life expectancy of the population has been extended less than three years between 1980 to 1996. That could not possibly account for the drastic increase of the cancer death rate within that time.
And third, increasing age need not be a factor, anyway-as the cancer-free Hunzakuts and Abkhazians prove quite conclusively
For a brief moment in 1986, the clouds of propaganda parted and a sun-ray of truth broke through into the medical media. The New England Journal of Medicine published a report by John C. Bailar III and Elaine M. Smith. Dr. Bailar was with the Department of Biostatistics at Harvard School of Public Health; Dr. Smith was with the University of Iowa Medical Center. Their report was brutal in its honesty:
Some measures of efforts to control cancer appear to show substantial progress, some show substantial losses, and some show little change. By making deliberate choices among these measures, one can convey any impression from overwhelming success against cancer to disaster.It is clear that the American Cancer Society-or at least someone very high within it-is trying to give the American people a good old-fashioned snow job. The truth of the matter is-ACS statistics notwithstanding-orthodox medicine simply does not have "proven cancer cures," and what it does have is pitifully inadequate considering the prestige it enjoys, the money it collects, and the snobbish scorn it heaps upon those who do not wish to subscribe to its treatments.
Our choice for the single best measure of progress against cancer is the mortality rate for all forms of cancer combined, age adjusted to the U.S. 1980 standard. This measure removes the effects of changes in the size and age composition of the population, prevents the selective reporting of data to support particular views, minimizes the effects of changes in diagnostic criteria related to recent advances in screening and detection, and directly measures the outcome of greatest concern-death....
Age-adjusted mortality rates have shown a slow and steady increase over several decades, and there is no evidence of a recent downward trend. In this clinical sense we are losing the war against cancer.... The main conclusion we draw is that some 35 years of intense effort focused on improving treatment must be judged a qualified failure.24
1. "Amer. Cancer Soc. Warns of Valley Quacks," The Valley News (Van Nuys, Calif.), Dec. 10, 1972.
2. As quoted in College of Mann Times (Kentfield, Calif.), April 26, 1972.
3. Letter from Mabel Burnett dated Dec. 18, 1972; Griffin, Private Papers, op. cit.
4. Walter H. Walshe, The Anatomy, Physiology, Pathology and Treatment of Cancer, (Boston: Ticknor & Co., 1844).
5. Ravdin, R.G., et.al., "Results of a Clinical Trial Conceming The Worth of Prophylactic Oophorectomy for Breast Carcinoma," Surgery, Gynecology & Obstet-rics, 131:1055, Dec., 1970. Also see "Breast Cancer Excision Less with Selection," Medical Tribune, Oct. 6, 1971, p. 1.
6. "Treatment Differences and Other Prognostic Factors Related to Breast Cancer Survival: Delivery Systems and Medical Outcomes," by Anna Lee-Feldstein, Hoda Anton-Culver, and Paul I. Feldstein, Journal of the American Medical Association, ISSN:0098-7484, April 20, 1994.
7. Hardin B. Jones, Ph.D. "A Report on Cancer," paper delivered to the ACS's 11th Annual Science Writers Conference, New Orleans, Mar. 7, 1969.
8. See "Results of Treatment of Carcinoma of the Breast Based on Pathological Staging," by F.R.C. Johnstone, M.D., Surgery, Gynecology & Obstetrics, 134:211, 1972. Also "Consultant's Comment," by George Crile, Jr., M.D., Calif Medical Digest, Aug., 1972, p. 839. Also "Project Aims at Better Lung Cancer Survival," Medical Tribune, Oct. 20, 1971. Also statement by Dr. Lewis A. Leone, Director of the Department of Oncology at Rhode Island Hospital in Providence, as quoted in "Cancer Controls Still Unsuccessful," L.A. Herald Examiner, June 6, 1972, p. C-12.
9. Johnstone, "Results of Treatment of Carcinoma of the Breast," op. cit.
10. National Enquirer, Oct. 7, 1973, p. 29.
11. Brunner, Emerson, Ferguson, and Doris Suddarth, Textbook of Medical-Surgical Nursing, (Philadelphia: J.B. Lippincott Co., 1970) 2nd Edition, p. 198.
12."Too Many X-Rays Increase Risk of Leukemia, Study Indicates," National Enquirer, Dec. 5, 1971, p.
13."Top FDA Officials Warn: Chest X-Rays in Mobile Vans Are Dangerous and Must Be Stopped," National Enquirer. Sept. 10, 1972, p. 8.
14. Fisher, B., et. aL, "Postoperative Radiotherapy in the Treatment of Breast Cancer; Results of the NSAPP Clinical Trial," Annals of Surgery 172, No.4, Oct. 1970.
15. "Preoperative and Postoperative Radiation Therapy for Cancer," speech delivered to the Sixth National Cancer Conference, sponsored by the American Cancer Society and the National Cancer Institute, Denver, Colorado, Sept. 18-20, 1968.
16. Breast Cancer Update/Q & A, by Ridgely Ochs, Newsday, December 19, 1995, p. B23.
17. Jones, "A Report on Cancer," op. cit.
18. Letter from Mrs. Glenn E. Baker, Executive Director, Southern District, ACS, addressed to Mr. T.G. Kent, reprinted in Cancer News Journal. Jan/Feb., 1972, p. 22.
19. Jones, "A Report on Cancer," op.cit.
20. Robert N. Proctor, Cancer Wars: How Politics Shapes What We Know and Don't Know About Cancer (New York: Basic Books, 1995), p. 4.
21. Letter from John Richardson, M.D., to G. Edward Griffin, dated Dec. 2, 1972; Griffin, Private Papers, op. cit.
22. Letter from Dean Burk to Frank Rauscher; Griffin, Private Papers, op. cit., p. 3.
23. Letter from Dean Burk to Congressman Frey; Griffin, Private Papers, op. cit., p.5.
24. "Progress Against Cancer?", New England Journal of Medicine, May 8, 1986, p. 1231
http://www.worldwithoutcancer.org.uk/hoax.html
http://www.curezone.com/diseases/cancer/cancer_surgery_statistic.asp
No comments:
Post a Comment